
Before & After Gallery
Amelia's Chesnut Journey

Meet Amelia, Age 33
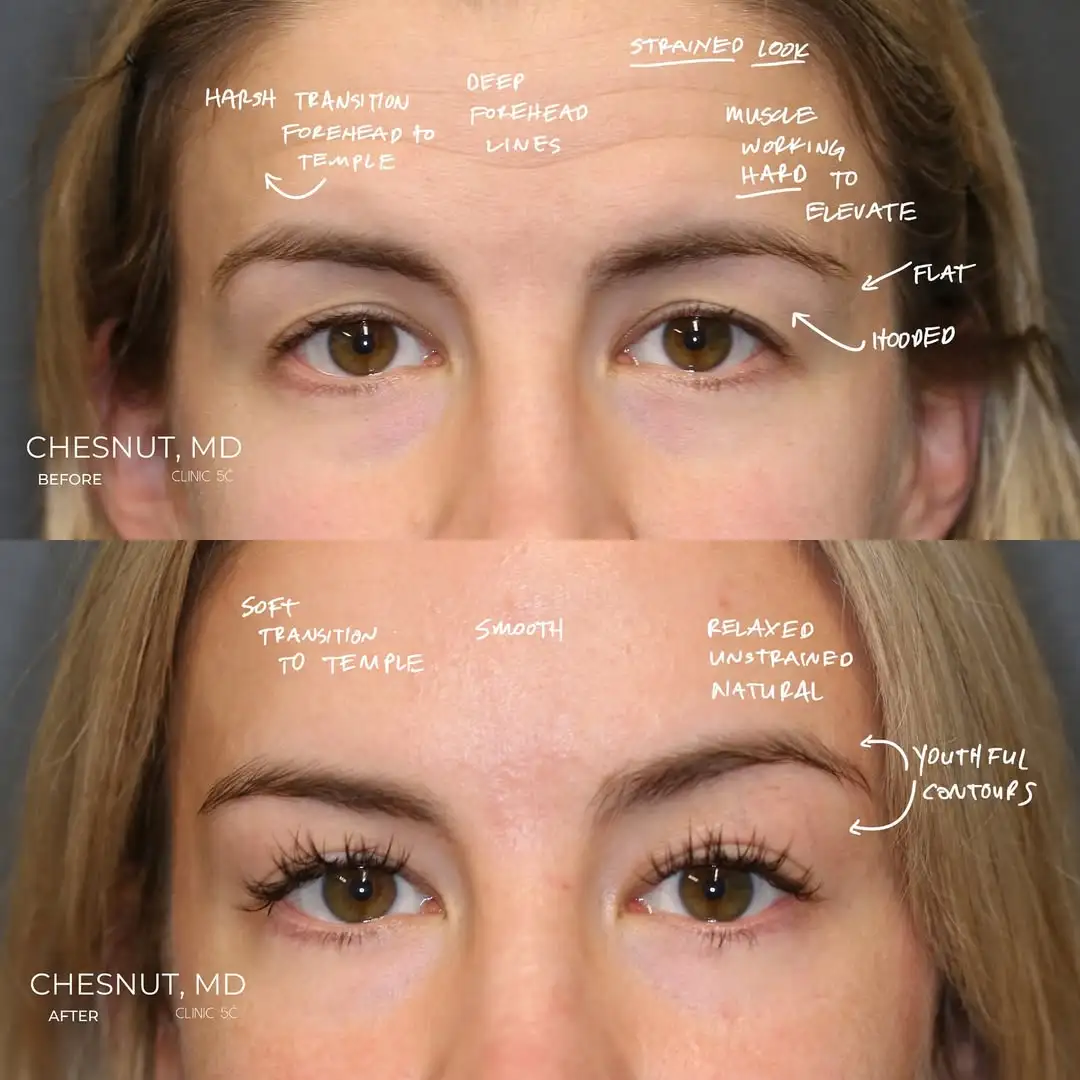
Amelia had spent her entire life working harder than she should have had to just to keep her eyes open. Not in the metaphorical sense, but literally: the weight of her brows required constant muscular compensation from the only muscle capable of lifting them, her frontalis, which she had been recruiting every waking hour for as long as she could remember. The result was a forehead etched with deep lines that had no business being there at 33, brows that sat unevenly depending on which side was compensating more on a given day, and upper eyelids that hooded in a way that made her look tired and heavy even when she felt neither.
She had tried to address it twice with Botox. Both times, the result made things worse. The lines did not resolve. The brows did not lift. Instead, the weight increased in some areas and peaked awkwardly at the outer edges in others, producing the characteristic oddly arched shape that emerges when the lifting muscle is weakened while the underlying structural problem remains entirely unaddressed. She left both treatments feeling more self-conscious than before.
What brought Amelia to the right consultation was a willingness to look past the familiar and find a solution that matched the actual anatomy of her problem. At 33, with a genetic and structural concern that had been present since her youth, she needed an approach built around what was true, not around what was conventionally offered first.
Amelia’s situation is one that appears in consultations with regularity, and the mismatch between what she had been offered and what her anatomy actually required is worth examining carefully, because it reflects a pattern that affects many patients who arrive having already tried the wrong solution.
Her forehead lines, her brow heaviness, and her hooded upper lids were genetic in origin. They had been present since her youth, they were structural rather than muscular, and they were being actively compensated for by her frontalis muscle working overtime to hold her brows in a position that allowed her to see clearly and present to the world without the full weight of her anatomy dragging her expression downward. The lines in her forehead were not a sign of aging. They were evidence of effort, specifically the effort of a muscle that had been doing a structural job it was never designed to sustain indefinitely.
Botox, in this context, is not just ineffective. It is counter productive. The frontalis is the only muscle capable of lifting the forehead. Weakening it in a patient who is already dependent on it for brow elevation does not produce a lift. It produces a drop, with the added complication that the outer portions of the brow, which tend to overcompensate relative to the central brow, may continue to pull upward while the rest descends. The resulting shape, an oddly peaked outer arch with a heavier central and inner brow, is sometimes called Spocking, and it is a recognizable consequence of applying a muscular relaxant to a problem that is fundamentally structural.
Amelia had experienced exactly this twice. The path forward required a different category of thinking entirely: not how to relax the muscle, but how to correct the structure that the muscle had been compensating for all along.
The surgical plan for Amelia was shaped by two governing principles. The first was anatomical correctness: address the actual source of each concern rather than its surface expression. The second was age-appropriate restraint: at 33, the goal was a relaxed, naturally contoured result that restored her face to what it should look like at this stage of her life, not a dramatic intervention that would look incongruous with everything else about her.
The sequence of the plan mattered as much as its components. The upper eyelid work came first, because establishing the correct eyelid position and symmetry provided the foundation from which the brow correction could be precisely calibrated. Correcting the lids without first addressing their relationship to the brow, or vice versa, risks producing a result that solves one part of the equation while leaving the rest unbalanced. The two zones had to be understood and treated as a system.
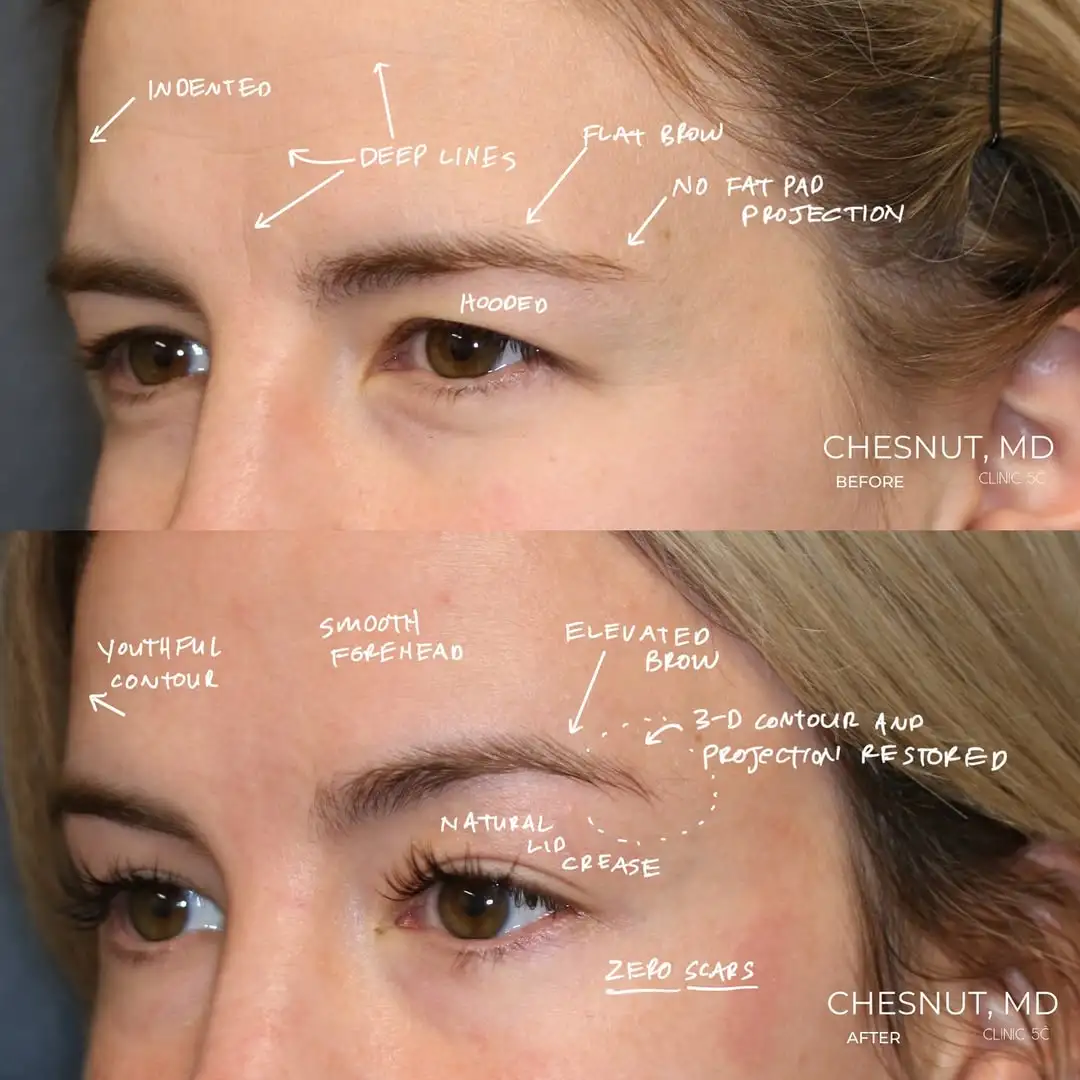
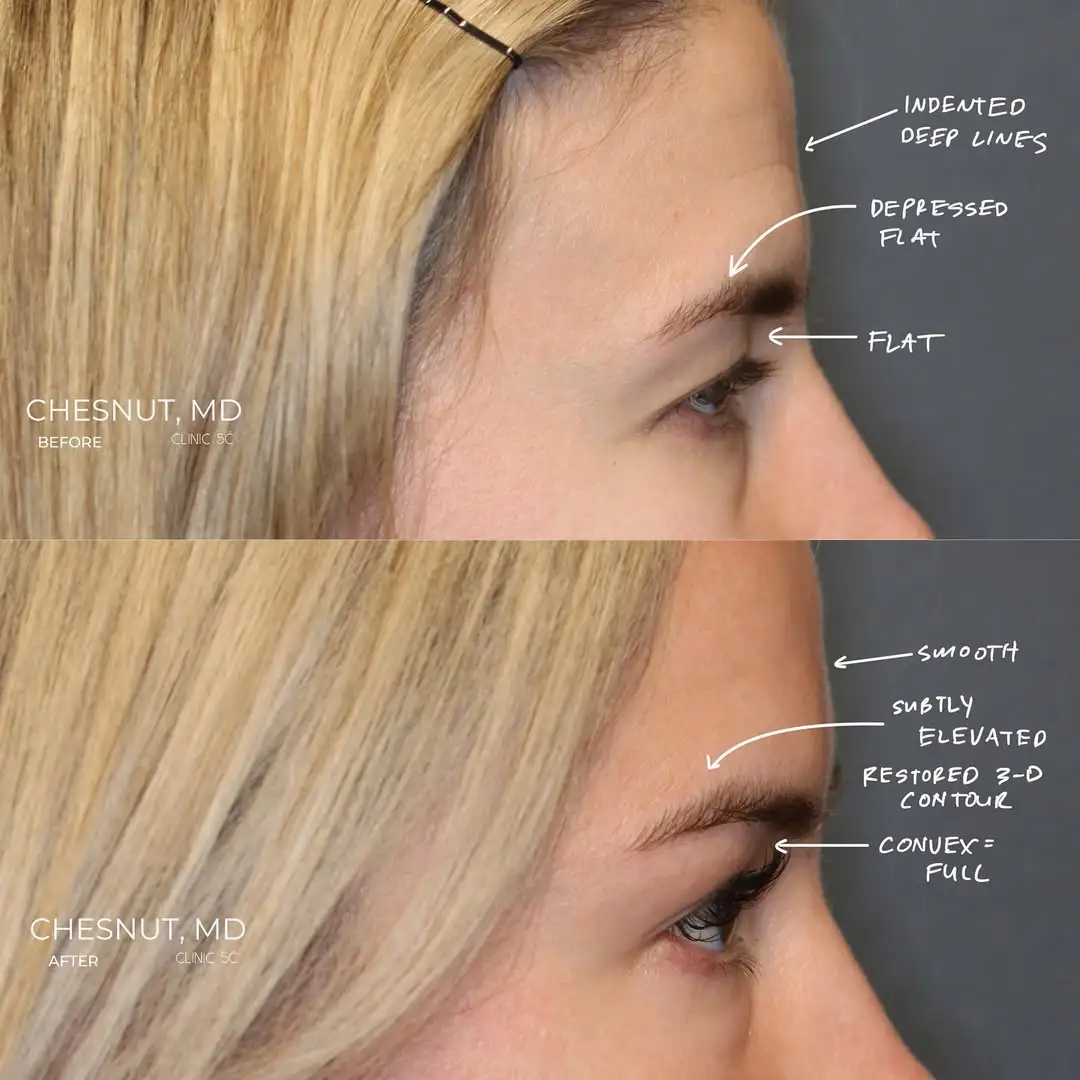
Her upper eyelid blepharoplasty was performed entirely without external incisions, a completely scarless approach that is genuinely uncommon in the field. The ptosis correction was similarly scarless. With the eyelid symmetry more foundationally established, the invisible access brow contouring elevated her entire forehead, releasing the frontalis from the constant load it had been carrying and allowing it to rest for what may have been the first time in her adult life. The deep forehead lines, which were the visible record of that sustained effort, would remodel over time as the muscle no longer needed to work against the structural weight above it.
Stem cell rich fat transfer completed the plan, restoring appropriate volume to the upper eyelid and brow area where years of hyperactive frontalis use had hollowed out the natural contour. Putting the fat pads back where they were supposed to be, both positionally and volumetrically, was the final element of a plan designed to return her face to the version of itself that her anatomy had always intended.
- Scarless upper eyelid blepharoplasty with no external incisions
- Scarless ptosis correction
- Invisible access Enigmalift brow contouring and forehead elevation
- Stem Cell Rich Fat Transfer for upper eyelid and brow volume restoration

At six weeks, the early results were already telling a clear story. The brows sat in a position they had never held without muscular effort. The upper eyelids were more open and more symmetrical than they had been throughout her adult life. The forehead, released from the constant compensatory lifting it had been performing, was beginning to soften. The deep lines that had made her appear decades older than33 were already less pronounced, and the healing process that would continue to remodel the tissue had only just begun.
The interplay between her forehead and her eyelids, which had been the defining dynamic of her pre-operative presentation, was now working in her favor rather than against her. With the structural weight of the brows addressed and the eyelid position corrected, the system that had been under sustained compensatory strain was finally in equilibrium. Her face, at rest, looked the way a 33-year-old face should look: relaxed, open, and naturally contoured without any suggestion of effort.
Four months brought the result into sharper focus. The brow position had stabilized. The upper lid symmetry was holding. The fat transfer had integrated, restoring the fullness in the upper eyelid and brow area that years of frontalis overuse had depleted. The forehead lines continued to remodel as the underlying cause of their formation was no longer present.
At eight months, the transformation was fully visible and the forehead remodeling was well underway.The harsh lines that had been etched into her forehead by decades of compensatory muscle recruitment had resolved to a degree that reflected both the structural correction of the underlying problem and the tissue’s own capacity to recover once the load driving the damage was removed. She looked like herself, at the age she actually was, without the burden of a structural problem she had been quietly managing her entire life.


At eight months, Amelia’s results were, by any reasonable measure, exceptional. The concerns that had brought her in were resolved. The structural problems that had defined her appearance since childhood were corrected. Her outcome was already more than she had imagined possible.
And yet, at her most recent visit, both patient and surgeon found themselves in a conversation about a small remaining asymmetry in her brows and whether to pursue a minor adjustment to address it. Not because the result was inadequate. It was not. But because the standard both of them were holding the outcome to was not adequacy. It was the closest possible approximation of perfection that the anatomy and the technique could produce together.
That conversation is worth acknowledging openly, because it reflects something true about how the best outcomes are approached. A 97 percent result is genuinely excellent. The question of whether to pursue the remaining three percent is not a simple one. It involves weighing the incremental benefit of a minor adjustment against the straightforward reality that any additional procedure carries its own recovery, its own variability, and its own uncertainty. Amelia and her surgeon were having that conversation honestly, with full information on both sides, which is exactly how it should be had.
The willingness to have it at all, to look at a result that most patients would consider a complete success and ask whether there is still something worth refining, is a reflection of the standard that had guided every decision in her care from the beginning. Not what is good enough. What is as right as it can possibly be.

A Structural Problem, Finally Solved
Amelia’s story is, at its core, about the difference between treating a symptom and correcting its cause. The lines in her forehead were a symptom. The brow asymmetry was a symptom. The hooded upper lids were a symptom. The cause, a genetic structural heaviness that had required constant muscular compensation since her youth, was the thing that needed to be addressed, and no amount of neuromodulator applied to the compensating muscle was ever going to reach it.
At 33, with the structural correction in place and the result still refining at eight months, Amelia’s face finally reflects what it should have looked like all along. Relaxed. Open. Naturally and appropriately contoured for her age. Without a single visible scar or access point to explain how it got there.
The forehead muscle that spent her entire life working overtime is finally at rest. Everything it was compensating for has been addressed. What remains is simply her face, doing nothing more than it needs to, looking exactly the way it was always meant to look.
.avif)
Ready To Start Your Journey?
Fax: (844) 961-3417