
Does Filler Actually Migrate? What a Surgeon Finds in the OR
By Dr. Cameron Chesnut | Five Codes Podcast | OR Diaries
The debate comes up constantly in aesthetic medicine: does dermal filler move from where it was placed? Some injectors insist the answer is almost always no. What looks like migration was simply placed there intentionally, or is "just normal tissue response," they say. I want to offer a different perspective, because I've seen the answer with my own eyes in the operating room.
This week I was performing a neck revision on a patient who had previously received lower face and chin filler. As I was working through the musculature of her neck, well below any area that would be a standard injection site, I encountered pockets of hyaluronic acid filler embedded deep within the muscle tissue. Not superficially. Not near the jawline. Down in her neck.
There is simply no reasonable clinical explanation for filler to be in that location other than migration. It moved there from where it was originally placed.
What Is Filler Migration?
Filler migration occurs when injected material travels from its intended placement site to an adjacent or distant area.
This can happen over days, months, or years, sometimes gradually enough that neither patient nor provider notices until it becomes visible, palpable, or is discovered incidentally during another procedure.
Hyaluronic acid (HA) fillers are hydrophilic, meaning they attract water, which affects their behavior in tissue over time. Combined with the constant movement of facial muscles, gravitational forces, and the path-of-least-resistance principle of soft tissue planes, migration is a documented phenomenon with a growing body of peer-reviewed evidence behind it.
A 2023 narrative review in Cosmetics identified 28 published reports of filler migration across clinical and observational literature. The affected patients ranged in age from 21 to 86, and hyaluronic acid was the most commonly implicated material.
For a deeper read: Chaput B et al. Filler Migration after Facial Injection: A Narrative Review. Cosmetics, 2023. (MDPI)
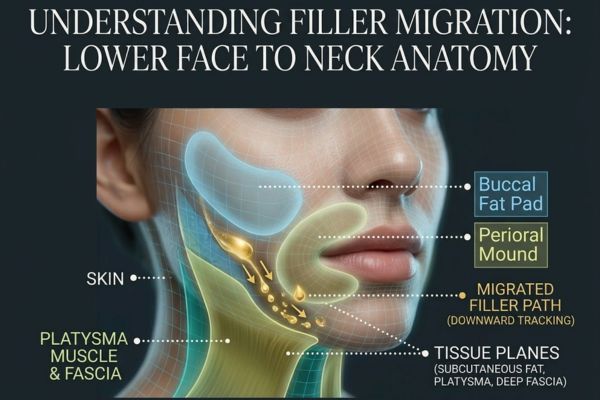
How Does Filler End Up in the Neck?
In this patient's case, the filler had been placed in the lower face, likely along the jawline, chin, and surrounding areas. Over time, the material tracked along the natural tissue planes of the face and into the neck musculature.
Facial anatomy creates predictable pathways. Gravity pulls soft material downward. Muscle movement creates pressure that can push filler along fascial planes. The lower face and neck are anatomically continuous, with no sealed barrier between them. When enough filler accumulates over time, with enough muscular force and gravitational assist, it can travel further than most patients or their injectors would expect.
This isn't a failure of any single treatment or a rare catastrophic event. It's a predictable consequence of the physics of soft tissue, compounded by years of cumulative volume.
For a deeper read: Rzany B & DeLorenzi C. Understanding, Avoiding, and Managing Severe Filler Complications. Plastic and Reconstructive Surgery, 2015. A key paper on filler mechanics and complication pathways. (PubMed)
The Compounding Problem: What Else Was in Her Neck
The migrated filler was only one layer of the problem. This patient had also undergone neck liposuction years earlier, the wrong procedure for what she actually needed. Her neck laxity called for lifting and structural repositioning, not fat removal. Instead, the subcutaneous fat that was removed was the very tissue doing an important job.
The subcutaneous fat beneath the skin of the neck isn't cosmetic excess. It's a functional glide plane. It allows the skin to move independently of the underlying muscle, maintaining the soft, natural appearance of a healthy neck. When that fat is removed aggressively, the skin and muscle can adhere to each other, creating fibrotic scarring, loss of natural movement, contour irregularities, and a hollowed appearance that is both aesthetically and structurally problematic.
By the time I was operating, the muscle in her neck had the texture of Swiss cheese, pocked with defects from the adhesion and fibrosis. I was separating muscle from skin, repairing the defects, removing the migrated filler, and then addressing the underlying structural problem that should have been treated initially.
This is a pattern I see in revision cases: a non-surgical treatment was chosen because it seemed less invasive, but it addressed a symptom rather than a cause and created secondary damage that made the eventual surgical correction more complex.
Why Neck Liposuction Is Often the Wrong Answer
This bears emphasizing because neck liposuction is commonly offered as a simple, minimally invasive solution for neck laxity or fullness. For the right patient, someone with genuine fat excess and excellent skin quality, it can be appropriate. But it is frequently applied to patients whose primary issue is not excess fat, but descent of structures that need to be lifted.
Injectable treatments like Kybella, which target submental fat, have largely failed for the same reason: they remove a tissue that often isn't the problem. Removing subcutaneous fat from a neck that lacks it creates hollowness, visible muscle banding, and skin irregularity. That is the opposite of the youthful neck contour patients are seeking.
The right question isn't "how do I remove what's there?" It's "why does this look this way, and what actually needs to move?"
Frequently Asked Questions
Does filler really migrate, or is that just a myth?
It is real and documented in the peer-reviewed literature. Whether it happens from a specific treatment depends on the type of filler used, the volume injected, placement depth and technique, the area treated, and the individual's tissue characteristics. That said, the claim that it "almost never happens" or that any filler found away from its placement site must have been placed there intentionally is not supported by the clinical evidence, nor by what surgeons find in revision operating rooms.
How far can filler migrate from where it was injected?
Most clinically documented migration is local, meaning the filler shifts into an adjacent tissue plane or region. However, cases exist of filler traveling significant distances over time, particularly when large cumulative volumes have been injected over years. The case described in this episode involved filler from the lower face and chin traveling into the deep musculature of the neck, a clinically significant distance that underscores how important the anatomy of facial tissue planes is in predicting where filler may ultimately end up.
How do I know if my filler has migrated?
Common signs include: fullness, puffiness, or firmness in areas that weren't treated; asymmetry that develops gradually over time; a sense that your face looks "heavier" or that your features have softened or shifted; and skin that feels uneven or lumpy below the surface. In many cases, patients become aware that something has changed but struggle to identify exactly what. A skilled surgeon evaluating your face can often identify migrated filler by palpation, and ultrasound can be used to locate material in deeper tissue planes.
Can migrated filler be removed?
Hyaluronic acid filler can be dissolved with hyaluronidase, an enzyme that breaks down HA. This is straightforward for superficial or accessible migration. For filler that has tracked deep into muscle or fascial planes, as in this case, surgical removal during a procedure may be the more complete option. Permanent fillers (silicone, PMMA, polyalkylimide) cannot be dissolved and must be surgically excised, which is one of several reasons why permanent fillers carry a substantially higher risk profile.
Was neck liposuction the wrong choice? Isn't it minimally invasive and therefore safer?
"Less invasive" does not mean "more appropriate." The right treatment is the one that addresses the actual cause of the problem. For a neck with genuine fat excess and good skin elasticity, liposuction can be the correct tool. For a neck where the issue is structural descent, including laxity of the muscles and ligaments that support the floor of the mouth, sagging of the submental structures, and loosening of the platysma, liposuction removes a tissue that was doing structural work, often worsening the underlying problem while creating new ones. The lesson isn't that liposuction is bad. It's that diagnosis has to precede treatment.
Listen to the Full Episode
This post is a companion to the Five Codes Podcast OR Diaries episode where Dr. Chesnut walks through both cases in detail.
🎧 Listen on Spotify | 🍎 Listen on Apple Podcasts | ▶️ Watch on YouTube
.avif)
Ready to begin your wellness journey?
Fax: (844) 961-3417